Abstract
Summary: Since the late 1990s, bed bugs of the species Cimex lectularius and Cimex hemipterus have undergone a worldwide resurgence. These bed bugs are blood-sucking insects that readily bite humans. Cutaneous reactions may occur and can start out as small macular lesions that can develop into distinctive wheals of around 5 cm in diameter, which are accompanied by intense itching. Occasionally, bullous eruptions may result. If bed bugs are numerous, the patient can present with widespread urticaria or eythematous rashes. Often, bites occur in lines along the limbs. Over 40 pathogens have been detected in bed bugs, but there is no definitive evidence that they transmit any disease-causing organisms to humans. Anemia may result when bed bugs are numerous, and their allergens can trigger asthmatic reactions. The misuse of chemicals and other technologies for controlling bed bugs has the potential to have a deleterious impact on human health, while the insect itself can be the cause of significant psychological trauma. The control of bed bugs is challenging and should encompass a multidisciplinary approach utilizing nonchemical means of control and the judicious use of insecticides. For accommodation providers, risk management procedures should be implemented to reduce the potential of bed bug infestations.
In recent years, bed bugs have undergone a major resurgence in the number of infestations, leading to clinical and control problems. This rise in activity is truly a global event, with increases in numbers of infestations reported for the Americas (153, 238, 246), Australia (99, 102, 104), Europe (37, 44, 170, 196, 232, 254), Asia (145, 149, 177, 282, 284), and Africa (227).
Although bed bugs have a long association with humans, for a period from the 1950s to almost the start of the 21st century, this pest had become relatively uncommon, particularly in the more economically advantaged nations. Not only was the reappearance of this pest unexpected, but the degree of the resurgence has almost been met with awe by many in the pest management industry. A survey of Australian professional pest managers in 2006 indicated that numbers of infestations rose by over 4,500% in the early years of the 21st century (102), comparable to what has been seen in other parts of the world (189, 246, 254). Bed bugs have become especially problematic in the United States, being reported in all 50 states; now, an estimated 1 out of 5 Americans either has had a bed bug infestation in their home or knows someone who has encountered them (220). Currently, there is no peer-reviewed published data on the actual prevalence of bed bug infestations across the United States. However, two of the largest pest control firms in the United States have released information on the most affected cities, based on the numbers of bed bug treatments undertaken by their respective companies, and this information corresponds well to hits on a dedicated bed bug website (http://www.bedbug.org.au). Despite limitations and potential biases in these data (), the information probably represents a moderately accurate indication of the current situation, with the most problematic cities being Chicago, New York, Detroit, Cincinnati, and Philadelphia ( and ). Data from New York City showed that the number of bed bug complaints to the city council rose from 537 in 2004 to 10,985 in 2009 (43). Thus, bed bugs have rapidly become a widespread societal pest, and the risk of exposure through normal daily life appears to be increasing. In addition to homes and hotels, infestations are appearing in the office and retail environment, in the health and transport sectors, and in cinemas; in fact, they can be found in almost any location where people sleep or sit (103).
The top 15 bed bug cities in the United States according to two large U.S.-based pest control companies and hits to a dedicated bed bug website
Relative hits from the United States by state to the website http://www.bedbug.org.au as determined by Google Analytics, 6 June 2011 to 2 November 2011, based on 18,672 hits (134).
What is particularly confounding about the resurgence is that it involves two species: the common bed bug, Cimex lectularius L., and the tropical bed bug, Cimex hemipterus F. The involvement of these two species makes the ascertainment of the reasons for this global resurgence more challenging.
Various factors have been postulated to be responsible for the resurgence. Resistance to carbamate and pyrethroid insecticides (45, 167, 171, 185, 209, 261, 284), and, more recently, to the organophosphates (171, 284), has been well documented for both species. Resistance to the organochlorines and pyrethrin has been known since the 1950s (57), and resistance to the organochlorines infers cross-resistance to pyrethroids due to their similar modes of action. The difference today, compared with the past, is that most recent bed bug populations carry pyrethroid resistance (261, 303, 325), and the vast majority of insecticide products currently in use belong to the pyrethroid group. Insecticide resistance is probably the key initiator of the bed bug resurgence, and resistant bed bugs have been disseminated worldwide through increased international travel. The latter has been borne out by genetic investigations using microsatellite markers and mitochondrial DNA sequence data, where bed bug populations from the eastern United States have heterogeneous origins suggestive of multiple introductions (303). In contrast, that same study found that within a single multiple-residential-unit complex, the level of bed bug genetic diversity from all infested apartments was low. This finding suggests that the entire building's infestation started from the introduction of a few bed bugs or, possibly, even a single female. Poor pest control has been implicated in the spread of an infestation from a single point source to more than 68 of 320 rooms within a staff accommodation block (104). Thus, it appears that imperfect pest-management-related practices have probably contributed to the magnitude of the bed bug resurgence. This includes the lack of training of pest control technicians in the eradication of insecticide-resistant bed bugs, the slow response of pest management industry associations to develop bed bug management standards for control, the failure of regulatory authorities to ensure that marketed insecticide products are efficacious against current field strains, and the difficulty in obtaining quality information on the efficacy of bed bug control products (102, 103). Clearly, the reasons behind the resurgence are multifactorial, and many other possible contributors were reviewed previously (239).
The implication of the huge upturn in the number of bed bug infestations is that people are increasingly being exposed to the insect and, as a consequence, the various associated health risks. This has prompted a number of recent clinical reviews (67, 72, 78, 106, 126, 130, 143, 144, 175, 287, 289), while contemporary clinical investigations have only just begun to emerge (241, 250). Despite numerous reviews, articles continue to present unsubstantiated scientific facts on bed bugs. This paper reviews the health impacts of bed bugs and both the direct clinical effects (notably the cutaneous reactions produced from the bite) and the indirect but far-reaching impacts while attempting to dispel some of the long-standing urban myths about bed bugs and their bites and clinical effects. This is preceded by a brief discourse on bed bug identification and biology, which is essential knowledge for the understanding of control and the reasons why the species is a public health pest. An overview of the control of this pest is also provided, given the challenges of eliminating bed bugs in the human environment.
Bed bugs are hematophagous arthropods of the family Cimicidae within the order Hemiptera. The Hemiptera include the true bugs, namely, those insects with specialized elongated mouthparts, with most of them being phytophagous (i.e., feed on plant sap), and include common garden insects such as aphids and cicadas. Members of the Cimicidae can be distinguished from other hemipterans by being flightless (although they appear wingless, in fact, the wings are reduced to short transverse scales), are ovoid and flattened in shape, and are all obligatory blood feeders on vertebrates (60). The adult males have a pointed abdomen, while the female abdomen is much rounder ().
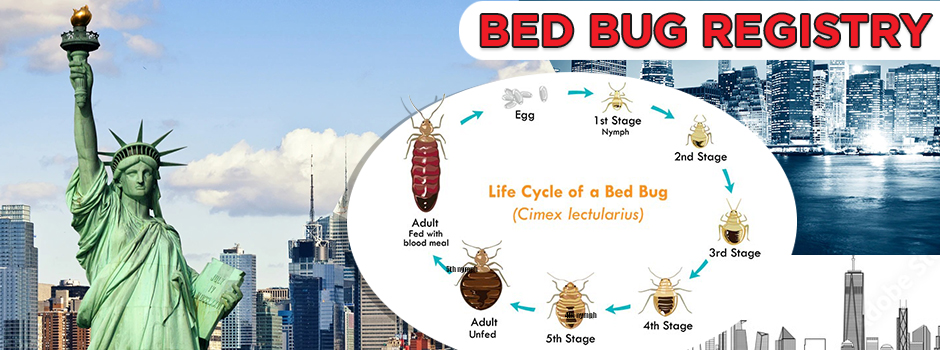
The various life stages of the common bed bug, Cimex lectularius. Bar, 5 mm. Depicted are the egg stage, the five instars, and both adults. All stages were identified according to the key of Usinger (297). (Reprinted from references 95 and 105.)
Of the 90 or so species within the family Cimicidae, only a handful bite humans, with the two main species being the common bed bug, C. lectularius, and the tropical bed bug, C. hemipterus. The common bed bug is aptly named; the Latin for the genus is bug, while for lectularius, it is bed (255). The two species are superficially similar, and samples should be referred to an experienced entomologist for identification. The species can be distinguishing by the presence of an upturned lateral flange on the margin of the pronotum on the thorax of C. lectularius, making the thorax relatively much wider than that of the tropical species (95, 297), although this feature is less obvious in the juvenile stages. In regard to their relative distributions, the tropical bed bug is confined mainly to approximately within the 30 latitudes (98, 102, 104, 216, 217), and the common bed bug is usually found outside this range (102). However, both species may appear beyond their normal ranges (104, 119).
The natural history of bed bugs has been reviewed in Usinger's seminal work, Monograph of Cimicidae (297), and more recently by Reinhardt and Siva-Jothy (252). The following section provides a brief overview of the biology of bed bugs.
In both bed bug species, there are five juvenile stages, called instars, which are miniature versions of the adults in general appearance albeit different in coloration (). The first instar is around 1 mm in length and off-white in color when unfed, becoming a deep red-brown and 5 to 6 mm long when unfed as fully grown adults (297). All nymphal stages and adults of both sexes require blood for nutrition and development, and it takes 3 to 10 min for complete engorgement to occur. The insects are attracted to the host by the carbon dioxide exhaled, body heat, and various compounds emitted across the skin, and they walk to feed off the host (bed bugs do not fly or jump). The preferred host is humans, but bed bugs will feed on other warm-blooded animals, including pets (71). In the United States, bed bugs (notably C. lectularius) can heavily infest poultry sheds, resulting in anemia and decreased egg production (63). Bed bugs tend not to live on the human body, and the only contact is for a blood meal, which occurs every few days if a sleeping host is available. Being a cryptic species (bed bugs are photophobic and thus quite secretive), blood feeding typically occurs at night, with peak feeding occurring between 1 and 5 a.m., when people are in their deepest sleep. During the day, bed bugs seek shelter in a variety of cracks and crevices and become inactive while digesting the blood meal. Bed bugs stay in close contact with each other and release aggregation pheromones to help relocate their harborage after a blood meal; this grouping also aids in water conservation (40). The presence of a harborage is indicated by fecal spotting (). Bed bugs also release alarm pheromones, which become most evident during the course of a treatment when the infestation is disturbed. The smell is very typically buggy in odor, which some authors often describe as being sickly sweet.
Bed bug infestation on a mattress. People most commonly encounter bed bugs in infested beds. The insects typically harbor along the mattress piping. Various stages can be observed, along with dark fecal spotting.
If a blood meal is continually available, the female C. lectularius bed bug will lay 5 to 8 eggs per week for 18 weeks at 23C and at 90% relative humidity (158), while C. hemipterus bed bugs will lay up to 50 eggs in their lifetime (150). It is often quoted that bed bugs can lay up to 500 eggs in their lifetime; however, this figure was based on one particularly highly fecund female C. lectularius bed bug that laid 541 eggs (297) and is atypical. The cream-colored eggs, which are elongated and around 1 mm in length (), are cemented onto rough surfaces of hiding places and will hatch within approximately 9 to 12 days at a room temperature of around 22C, but hatching will take longer under cooler conditions.
The length of the life cycle is extremely variable and is dependent on ambient temperatures. Under cool conditions of 10C, once-fed adults of C. lectularius can live for up to almost 485 days, while C. hemipterus can live up to around 300 days (226). These lengthy periods would generally not normally be observed, as under average home and hotel living conditions at temperatures of around 22C, the life cycle of both species takes around 2 months to complete, and the adult lives for up to a maximum of 4.5 months (58).
Encounters with bed bugs occur mostly commonly when people sleep in infested beds (), and often, the furniture and furnishings in the same room will also be harboring the insect. However, bed bugs can infest almost any site that people frequent (95).
The most common clinical consequences of bed bugs are the direct cutaneous reactions from the bite. The possibility of bed bugs acting as vectors for various infectious agents has been mentioned in the literature, although there is often little supporting evidence. There are other health impacts of bed bugs: the challenge and costs of pest control often lead people to desperate and dangerous acts; infestations have closed down hospitals, threatening the provision of health services; and bed bugs present various social issues. The mental health consequences of having an infestation are potentially serious (and may encompass delusions of parasitosis) but are poorly understood.
Bed bug mouthparts are adapted for piercing the skin and sucking blood and have extremely fine needlelike stylets that are inserted into the skin and are withdrawn after feeding. During feeding, the bug injects saliva that contains various protein fractions, some of which have anticoagulant properties. In C. lectularius, this includes nitrophorin, which is a vasodilator inducer (301); apyrase, which inhibits platelet activation and aggregation (299); and an inhibitor of factor X, which delays blood clot formation (300). A recent investigation on the sialome (saliva) of C. lectularius revealed 46 different protein components (116): many play a role in overcoming host hemostasis, some function in host protection (including possibly as antimicrobial agents), and others have a role that is as yet unrecognized. It has been stated that bed bugs inject an anesthetic, although none has yet been identified.
The salivary components of C. hemipterus have undergone only limited study. It has been found that this species contains a small amount of hemeproteins and has reduced anticlotting activity compared with C. lectularius, although the total protein contents of the saliva were similar between the two species (34). It is unknown if there are differences in salivary components between the instars or the sexes of either species.
After the removal of the stylets, some oozing at the bite site may occur, seen on bed sheets as small flecks of blood (276). Bites are often reported as occurring along the arms and legs but will occur on any area of exposed skin (241), although clothing can inhibit bites (241, 279).
The severity of cutaneous reactions from a bed bug bite varies between individuals. It is important that published bed bug bite descriptions have been based on a single observation as a one-off clinical presentation, and the source of the bite (as in bed bug instar, stage, or species) is usually not known, not identified, or not stated. Some individuals will develop no reaction, although this may depend on previous exposures (129, 250). The reaction may start out as small indistinct red macular lesions less than 5 mm in diameter (130) (), which may later progress into large circular or ovoid wheals (77, 79, 280), usually described as papular urticaria (although they may last for more than 24 h and should not be regarded as urticaria), and may be as big as 2 to 6 cm in diameter, which represents the more classic bed bug wheal. These lesions tend to be intensely itchy ( and ). Although the wheals have been reported to be up to 20 cm in diameter (72), those authors did not cite their original source, and it is possible that such reactions could have resulted from multiple bites or from trauma at the bite site through scratching, thereby increasing the size of the lesions. Pseudopodium-like extensions of erythema around the periphery have also been noted (70), which may correspond to livedo-like patterns. It has often been stated that a small hemorrhagic punctum can be at the center of the bite mark at the time of the bite (70, 79, 266), but this has not been observed in our experience. If there are large numbers of bed bugs (), the individual lesions can coalesce to give the appearance of a more generalized rash, possibly enhanced by trauma, such as scratching, to the affected areas (), complicating the differential diagnosis (49, 70, 194, 267, 287). If the bed bug infestation is unrecognized or not treated, the cutaneous reactions can become chronic (46, 73), and dermatitis outbreaks from bed bug bites have been reported in health care facilities (81). Bite reactions can take some weeks to resolve (130), depending on the severity of the reaction. Patients with multiple bites or a severe cutaneous reaction may develop systemic symptoms, including fever and malaise (182), although this appears to be rare (42).
Bite reactions the morning after being bitten by bed bugs. The bites are faint erythematous macules and papules 2 to 3 mm in diameter. The bed bug species was not identified; the bites occurred in a region where both C. lectularius and C. hemipterus occur. (Reprinted from reference 105.)
Same patient shown in but 4 days later. Lines of bites that run along the body can be observed, along with the classic bed bug wheal, measuring 2 to 3 cm in diameter. (Reprinted from reference 105 [courtesy of Nigel Hill].)
Lines of bites along the arm. The bed bug species was not identified.
A 4-year-old girl bitten by hundreds of C. lectularius bed bugs (identified by the authors). Multiple discrete bed bug wheals, some with purpuric centers, cover much of the body. (Reprinted from reference 105.)
Same patient shown in . A diffused erythema has developed in the more severely bitten areas. This could be the result of trauma (e.g., scratching) to the affected areas.
Vesicles and bullae containing clear or bloody exudate that appear some days following a bite have been reported (75, 115, 172, 181, 182, 266, 279, 288) (). The frequency of bullous eruptions is unknown; it has been stated that they are uncommon (182), but an investigation of bed bug bites on passengers on a tram found eight patients who all developed such eruptions on the legs (172).
Bullae with hemorrhagic serum on the hands and ankles from the bite of C. lectularius (identified by the authors). These appeared between 24 and 36 h following the bites. The purpuric/necrotic lesions on the ankle indicate the severity of the reaction. (Reprinted from reference 105.)
The immune basis of the clinical reaction is largely uncertain. In one study of 15 patients with papular urticaria, all had IgG antibodies to C. lectularius antigens, although as whole ground dried salivary glands were used as the antigen, the antibody responses to the individual antigenic proteins were not identified (1). Nitrophorin has been shown to induce allergen-specific IgE antibodies in one patient hypersensitive to the bite (181). Similarly, the pathological changes in the skin from a bed bug bite have been poorly studied. Biopsy specimens of the bites show edema present between the collagen bundles in the dermis, with lymphocytes and numerous eosinophils being present around the blood vessels (73). Epidermal spongiosis and inflammatory infiltrate in the upper and lower dermis around vessels and epidermal adnexal structures, a perivascular inflammatory infiltrate in the papillary dermis, and lymphomononuclear cells and numerous eosinophils around the vessels and between the collagen fiber bundles have all been observed (78). Intra- and subepidermal bullae with an inflammatory infiltrate composed mainly of lymphocytes, histiocytes, and some neutrophils and eosinophils have also been noted (288). However, the correlation of specific histopathological findings with the timing of the initial bites is limited, and further investigation is needed.
There are limited data on the percentage of individuals reacting to bed bug bites. Most reports were of isolated observations rather than prospective clinical studies of the change in reactions when patients are exposed to bed bugs repeatedly over time. Reinhardt and colleagues (250) reviewed the literature on human reactions to bed bug bites, and when data from all the studies were combined, 249 out of 331 (75%) patients developed a reaction. However, those investigations were not directly comparable; some involved placing bed bugs on volunteers to record the reaction, some undertook repeated exposures to measure changes in reactions over time, and other studies noted cutaneous reactions in people within infested premises (i.e., isolated patient observations).
The largest of the early studies was undertaken at an internally displaced-person camp in Freetown, Sierra Leone (119). Of 221 individuals living with bed bugs, 196 (86%) had wheals from the bites, although it was not stated what percentage of the individuals had previous exposure to bed bugs. The study was further complicated in that both C. hemipterus and C. lectularius coexisted in the camp, and no attempt was made to distinguish the relative clinical reactions from the two species. To date, no study has compared the differences in clinical reactions from the bites of the two species.
Most contemporary studies have reported only the effect of C. lectularius bites. In a prospective clinical study of volunteers bitten by C. lectularius bed bugs, it was found that 18 of 19 patients (94.7%) developed a skin reaction albeit often only after repeated exposures (250). With the first bites, 13 of 24 patients (54.2%) had no reaction. The period for the bite reaction to appear decreased from around 10 days to a few seconds following repeated bites (250).
The most comprehensive study of reactions to bed bug bites involved 474 individuals in the United States, all with an independently confirmed infestation (241). The species of bed bug was not stated, although it is assumed to be C. lectularius, as there have been no reports of C. hemipterus from the U.S. mainland (as stated above, C. hemipterus occurs mainly within the 30 latitudes). Seventy percent of respondents (raw data not given) reported skin reactions, although none were confirmed through cutaneous examination by a medical practitioner. Respondents over the age of 65 years reported a lower reaction rate (42% claimed no reaction). While the sample size was not considered significant, a similar level of no reaction (41%) was recorded for children between 1 and 10 years of age. Around half of those surveyed stated that they had the infestation for 1 month or less, and so it is probable that some had yet to develop bite sensitivity.
Some individuals may not develop a reaction, even with repeated exposures. Goddard reported feeding 15 C. lectularius on himself every 3 weeks over a 6-month period, yet no cutaneous or clinical reaction developed (129).
Bed bug bites may appear in a linear fashion, either individually or as groups. A number of authors have stated that the bites appear in groups of three, colloquially referred to as breakfast, lunch, and dinner (67, 73, 78, 143, 175, 289, 326). To date, the distribution of bites on patients has not been quantified or analyzed. Even when authors have pointed to a group of three bites on a photograph of a patient within a publication, this pattern is not often obvious and certainly not evident for all bite patterns (78).
We have reviewed images sent to our laboratory of 30 patients with clinical bite reactions to bed bugs, and a pattern of three was difficult to discern. Bites were often singular and somewhat random, in groups of two or more, and often in lines, or there were so many bites that a widespread rash was hiding individual bite reactions. At least one other author has questioned the often-quoted three-bite relationship and similarly observed that bites are often arranged in rows or clusters (79). The concept of breakfast, lunch, and dinner bite clustering may be just one of the many myths surrounding bed bugs.
In reviewing the same 30 patients, a linear pattern of bed bug bites was often obvious when there were multiple bites and frequently on a line of 30 cm or more in length ( and ). It should be noted, however, that many of the bites seemed to be randomly situated. There are at least three possible explanations for the lines of bites:
The insects are test biting and do not always locate a readily flowing vein or capillary on the first probe
The feeding is interrupted by the movement of the host, and the bed bug resumes feeding after the sleeping victim settles (38)
Many bed bugs are biting along the one line.
In the case of explanations 1 and 2, these would not necessarily explain a line of bites, unless the biting occurred along a blood vessel line. Also, as the line of bites can cover some distance, it is not intuitive that an insect moves away some distance before refeeding or test feeding. Once a bed bug starts feeding and the stylets are implanted, it takes quite some physical disturbance for the insect to dislocate and move. From data from the 30 patients mentioned above and from other published images of bed bug bites (5, 73, 78, 178, 267, 280), it is evident that there tends to be a general direction to the lines of bites; they tend to be along the limbs rather than across and vertically along the torso rather than across. On the shoulder, lines of bites often run along the collarbone region. Thus, the direction of the bite lines appears not to be random.
As stated above, bed bugs release aggregation pheromones such that they tend to harbor in groups. Presumably, when blood feeding, a number of bed bugs from the same harborage would move in a general direction toward the recumbent sleeping host. Bed bugs, while feeding, sometimes keep the body in contact with the bedding and project the mouthparts forward into the skin (H. J. Harlan, unpublished data). A line of bites could then be the result of a number of bugs feeding on the patient during sleep over an area, with the line being coincidental and merely a result of the limitation of where the bugs can reach from the bedding. This hypothesis would explain the directional nature of the bites along the limbs and torso.
Another controversial issue is the times often cited in the literature for a bed bug reaction to appear. Historically, a delayed reaction of up to 9 to 10 days has been reported (266), although most patients tend to show observable clinical signs within 24 to 48 h or even within minutes in hypersensitive individuals (250). Bed bugs are highly secretive insects that are most active at night, and many patients would not notice the presence of the insect, especially if the infestation is relatively light. As the insect can be transferred in luggage, furniture, and other belongings, the first sight of the insect may not represent the initial encounter, especially while people are traveling. Patients may not develop an allergic response upon the first exposure to the bite but often do so upon a subsequent exposure. A new bite, while the sensitivity reaction to an earlier bite is developing, may be confused with the appearance of a delayed reaction. Thus, there could be doubts about some of the earlier times cited in the literature for the appearance of reactions. In the prospective clinical study mentioned above by Reinhardt and colleagues (250), it took up to 11 days for many patients to develop their first reaction, which does coincide with data from earlier reports.
There are no reports relating to patients known to be sensitive to the bite of either C. lectularius or C. hemipterus regarding whether they would develop a similar lesion when bitten by the alternative Cimex species. Usinger (297) commented on his own cutaneous reactions when feeding various species. After feeding C. lectularius on himself for 3 years, a bite from Cimex pilosellus (Horvath), a bat-feeding species, produced an immediate reaction similar to that of C. lectularius. Hesperocimex sonorensis Ryckman (a bird-associated species) also produced an immediate reaction but of a different clinical appearance, while Leptocimex duplicatus Usinger (another bat feeder) produced no clinical reaction with the first bite and a mild reaction upon subsequent bites. Usinger concluded that the degree of clinical cross-reactivity was dependent on the relationship of the various species; the two Cimex species produced evidence of a cross-reaction, whereas the more distantly related Hesperocimex and Leptocimex had either a different or no reaction.
Cimex lectularius and C. hemipterus are very closely related species. In both the laboratory and the field, the two species will undergo interspecific mating (215, 307), even occasionally producing a species hybrid (214). Thus, it could be presumed that the antigenic compounds within the saliva would be similar and produce comparable clinical cross-reactions in patients sensitive to the bite of either species. However, as discussed above, there are some differences in salivary compounds between the species, with C. hemipterus having fewer hemeproteins (34). The senior author (S.L.D.) has a known sensitivity to C. lectularius bites, yet when he fed an adult female C. hemipterus to repletion (i.e., full engorgement) for the first time, no clinical reaction was observed (S. L. Doggett, unpublished data). Of course, this represents only a single observation, and further investigations are required to confirm if this is a general phenomenon. However, perhaps C. hemipterus is lacking the salivary proteins of C. lectularius that induce the antigenic response, but the reverse may not hold true, and a sensitivity to C. hemipterus may result in a reaction to C. lectularius bites. Further research is required in this area.
Insect bites are generally difficult to definitively identify and characterize, and the bite reaction can vary tremendously between individuals, even for the same insect species. This makes accurate diagnosis and management challenging (137). A single bite from a bed bug, particularly soon or some time after the bite, is not easily identifiable as being caused by that insect. The development of a wheal may suggest that bed bugs are present, and a line of bites along the limb may provide further circumstantial evidence. Ultimately, a positive insect identification is the only sure way of definitively diagnosing the cause. A thorough inspection of the home, particularly around sleeping areas or in the locations suspected to be where the bites were acquired, by an experienced pest manager should be undertaken to confirm the presence of bed bugs and to exclude other possible biting arthropod pests (91). One report suggested that bed bugs should be considered for the differential diagnosis of patients who present with mysterious skin rashes (128).
It is not uncommon to misdiagnose the bite of bed bugs as scabies (278) (which should always be confirmed by a skin scraping), antibiotic reactions, food and other allergies, mosquito or spider bites, chicken pox (105), Staphylococcus infections (133), allergic skin reactions (4), and prurigo (111). In one case of an anaphylactic reaction following a bed bug bite, the patient was initially diagnosed with a coronary occlusion (230). Misdiagnosis may result in inappropriate medical treatments, such as the use of scabicides (278), lesion biopsy specimens, and various other investigations (133).
If misdiagnosed, the bed bug infestation may continue and become firmly entrenched, with the risk of further spread. For example, in one instance, a child was suspected to have been suffering for 3 months with hives before the pest was identified, with the bugs being found only when the mother checked the child during the night and saw the bugs feasting (131). In another example, a 10-year-old girl went through a continuing nightmare of biopsies, blood tests, and ointments for over 6 months (133). The parents suspected bed bugs only following an Internet search, which led to the child's room being inspected at night and the cause of that misery being identified. One woman who was suffering ongoing skin reactions discovered the cause only after she heard media discussion of bed bugs; suspecting the worst, she lifted the mattress cover and was horrified to find literally thousands of bed bugs residing on her mattress (92). Another report recounted the tale of a woman who was being treated for scabies by her dermatologist and found out about bed bugs only after a conversation with a neighbor (278). In one unusual case, eight women developed a zone of raised spots across the back of their calves in almost identical positions. Investigations found two things in common: all traveled on the same tram, and all wore skirts. Upon inspection, the seat cushions were found to harbor bed bugs. The bugs could access only the exposed legs of women in skirts, which coincided with the position of the bite marks (172).
On the other hand, there are dermatologic diseases that may be misdiagnosed as bed bug infestations, such as Grover's disease, miliaria, prurigo, dermatitis herpetiformis, or acral papular or papulovesicular dermatitis of Gianotti-Crosti (73, 289). The differential diagnosis of bed bug bites depends on the morphology of the skin lesions and can be quite extensive. In delusions of parasitosis, the patient has the conviction that the skin is infected by parasites, and bed bugs can be one of the most commonly blamed arthropods. In cases where the clinical diagnosis is difficult, a skin biopsy is usually helpful to differentiate most dermatologic diagnoses from insect bites (73, 289).
Treatment regimens and outcomes for dermatological reactions to bed bug bites have been recently reviewed (130). There are no specific treatments (144), and the clinical reactions tend to be treated empirically as per other insect bites. For cutaneous reactions, topical steroids are used to control inflammation, and systemic antihistamines can provide relief from itching (130, 147, 262). Antibiotics or topical antiseptic lotions may be prescribed if secondary bacterial infections are present (276) or when the risk of secondary bacterial infections is high, e.g., those with numerous bites and skin excoriation due to scratching (142). Generally, however, antibiotic therapy is not required for otherwise healthy individuals, although good dermal hygienic practices are recommended (276). For patients who develop severe systemic reactions and anaphylaxis, intramuscular epinephrine, corticosteroids, and antihistamines may be required (130).
Even without treatment, symptoms tend to disappear within 1 to 2 weeks once the bed bug infestation is eradicated, as the bites are self-limiting (78), and the insect does not infest the skin. Scarring appearing as a deeper-colored skin tone may remain for some weeks to months (Doggett, unpublished). For individuals with severe anxiety or a secondary delusional infestation-like syndrome (117) associated with bed bugs, psychological therapy may be needed.
No bed bug allergens are available for desensitization programs for people who have severe bite reactions, although recent research into the bed bug sialome may identify appropriate allergens (62). Ultimate relief from bed bugs can be achieved only through the eradication of the active infestation.
Sleep deprivation is commonly associated with bed bugs (105, 130, 241). In a survey of 474 individuals with a bed bug infestation, 29% claimed insomnia or sleeplessness (241). Patients can awake during the night because of the bite's itch, and scratching can exacerbate the itch sensation, leading to greater sleep disturbance (known as the itch-scratch cycle) (291). Some patients have disturbed sleep from just the knowledge of having an active or past infestation in their own bed. Vandam (302) cited an example of a woman who would wake up in the night and place her pillow into the freezer. Sleep deprivation is a serious medical problem that can affect neurocognitive functioning, emotional status, and various physiological factors and may contribute to long-term health problems such as coronary heart disease (272, 314). Sleep loss is considered to have a major economic impact, and some of the most serious human-caused disasters (e.g., Three Mile Island, Chernobyl, and the grounding of the Exxon Valdez) have been attributed to a lack of sleep (74). No study has quantified the impact of bed bug infestations on sleep outcomes and its associated economic impacts; this needs investigation in light of the increasing frequency of infestations.
Various secondary bacterial infections as a consequence of the scratching of the bed bug bite site have been recorded, including cellulitis, impetigo, ecthyma, lymphangitis (54), and folliculitis (130). How widespread and common these secondary infections are is presently unknown.
There is a single report from 1922 reporting that liquid excreted from bed bugs during feeding can induce a urticarial reaction (237). It was also stated that chronic bed bug infestations can cause nervousness, lethargy, pallor and diarrhea (287); however, it is not clear if these symptoms are due to the bed bug bites or the mental trauma associated with having an infestation. It was also reported that repeated bed bug bites may produce a severe reaction with serum sickness (287), but, again, the frequency of this reaction is unknown.
It is not surprising that bed bugs are often lumped together with other hematophagous arthropods and suspected of being vectors of various pathogens. In the preantibiotic era, numerous investigations were undertaken to find a possible link between various diseases and bed bugs. The race to find such associations may even have influenced research outcomes, particularly when reviewed in the context of modern medical knowledge. Studies up to the early 1960s (around 75% were from between 1911 and 1940) were reviewed by Burton (55, 56), who described some 43 human diseases suspected of being transmitted by bed bugs. Of these, all but 6 were pathogen related and included examples of bacteria, rickettsia, viruses, protozoans, and nematodes. With the current understanding of vector-pathogen dynamics, as discussed below, some of the implicated organisms must be viewed with a high degree of suspicion. The nonpathogen disease associations included beriberi, pellagra, and cancer and must be treated with some skepticism. Burton did admit that several of the claimed associations were based on inference, deductive reasoning, or conjecture and were therefore not based on statistical epidemiology, microbial or vector investigations, or experimentation. Many of the reports cited were the result of the detection of a pathogen within bed bugs, but this does not mean that the insect is capable of transmitting the agent. In fact, there is no current evidence to suggest that bed bugs transmit any pathogen (124126).
Subsequent to the reviews by Burton (55, 56), there was a decline in the research interest in bed bugs as potential disease vectors, presumably due to reduced infestations following the widespread use of the highly effective insecticide dichlorodiphenyltrichloroethane (DDT).
Later projects relating to the potential vector status of bed bugs often coincided with research trends on certain human pathogens. In an era of intense investigation on filariasis in the 1960s, a number of papers examined the potential of bed bugs to transmit the causative filaria Wuchereria and Brugia. Despite wild-caught bed bugs being found to be infected with filarial worms, experiments failed to demonstrate transmission (55).
From the mid-1970s to the early 1990s, interest in blood-borne viruses, notably hepatitis B virus (HBV) and human immunodeficiency virus (HIV), sparked a number of investigations examining their possible transmission by bed bugs. As this was an area of intense research, the investigations are reviewed herein with some detail. Initially, it was noted in parts of Africa that there were high rates of HBV coincident with large numbers of bed bugs, and the rates of transmission within the community could not, at the time, be readily explained (165). The first suggestion that bed bugs may have a role in HBV transmission occurred during the early 1970s, when HBV surface antigen (HBsAg) was detected by radioimmunoassay (RIA) in 1 out of 18 pools of engorged bed bugs (species not stated) from the Ivory Coast (51). Collections of C. hemipterus on four separate occasions from villages in Senegal found HBsAg in nonengorged nymphs and adults in all four collections, with a total of 15 bugs positive by RIA out of 143 tested (321). At one of these sites, the occupant was known to be HBsAg positive. In a field investigation from the Northern Transvaal in Southern Africa (165), some 1,368 C. lectularius bed bugs were collected and tested in pools by HBsAg RIA. Thirty-two out of 140 pools contained HBsAg, with an average infection rate of 30.6/1,000 bugs. Both engorged and nonengorged bugs were HBsAg positive, with the latter suggesting possible transstadial transmission (i.e., from one nymphal instar to the next stage).
In laboratory investigations, Newkirk et al. (218) found that HBsAg could be retained in C. lectularius for 5 weeks and was maintained transstadially. Those authors also noted a change in HBsAg levels, suggesting the possible replication of the virus. However, they were unable to detect HBsAg in feces or eggs, with the latter suggesting a lack of vertical transmission. No attempt was undertaken to determine if HBV was still infectious or if bed bugs could transmit the virus via feeding on an HBV-negative host. In an almost identical experiment, the potential of HBV to be maintained in tropical bed bugs was examined, and HBsAg was found to persist for up to 6 weeks postfeeding (225). Again, no transmission studies were undertaken. Some years later, using molecular techniques, HBV DNA was detected in C. lectularius and feces for up to 6 weeks after feeding on HBV-infected blood (273). The authors of that study also tested the possible persistence of hepatitis C virus (HCV), but HCV could not be maintained within the bed bug. Other researchers employing molecular techniques found that HBV DNA persisted for up to 35 days in bed bug bodies and could be detected in feces for the same period and that the virus could be maintained transstadially through only one molt.
The first experiment testing the ability of C. lectularius to transmit HBV was undertaken via artificial blood-feeding devices (membrane feeders) and on laboratory animals (162). Transmission did occur albeit at very low rates. For the membrane feeders, HBsAg was detected in 3 of 35 bed bugs tested, while for the laboratory animals, HBsAg antibodies were detected in 2 of 10 guinea pigs and l rabbit. Those authors concluded that biological transmission was unlikely and that transmission was probably mechanical in origin. That study did show that HBsAg could persist for at least 7.5 weeks but that transstadial transmission was inefficient, with antigen being maintained for only one molt. Similarly, a transmission study with C. lectularius involving artificial feeding via membranes also found a very low rate of transmission, with only 1 of 7 serum samples in the membrane feeder testing HBsAg positive (285). In comparison with the above-mentioned study, the authors of the latter study concluded that HBV replicated within the bed bug. Those authors also reported a much longer period of HBsAg detection: up to 122 days postfeeding. Again, there was no evidence for the vertical transmission of HBV. It was subsequently demonstrated that HBsAg could be excreted in the feces by C. hemipterus (224). This finding suggested that, perhaps, the transmission of HBV through contact with infected bed bug feces may occur, although virion infectiousness was not examined.
In examining possible modes of transmission, Jupp and colleagues (164) concluded that the biological multiplication of HBV in bed bugs was not occurring, because virus loads decreased over time in bed bugs fed on HBV-infected blood. This finding was further strengthened by the lack of HBV in the salivary glands, as examined via electron microscopy in C. lectularius bed bugs that had been infected orally with HBV (163). The conclusion was that transmission was most likely to be mechanical and to occur through the crushing of live HBV-infected bed bugs, via contact with contaminated feces, or through interrupted feeding and/or regurgitation. Those authors also reported finding hepatitis E virus (HEV) antigen in wild-captured C. lectularius bed bugs collected from the Northern Transvaal, but transmission rates were much lower than those found for HBV. In India, HEV was also detected in bed bugs (292).
Arguably, the most compelling transmission research to date involved the feeding of HBV-infected C. lectularius bed bugs on three susceptible chimpanzees (166). Despite the monitoring of the chimpanzees for HBV antibodies for almost 1 year, none indicated infection, suggesting that transmission did not occur.
Epidemiological investigations examining possible associations between HBV-infected individuals and bed bugs are scant. For Gambian children under 5 years of age, there was a significant association between bed bugs in the beds and hepatitis B e antigen (HBe) antigenemia (198). Another report noted that there were high rates of HBV infections in a group of former prisoners of war held by the Japanese during World War II, and many had been heavily exposed to biting insects such as bed bugs and mosquitoes (123). The epidemiological link between bed bugs and HBV in these cases is by inference only. Following the initial epidemiological investigation in the Gambia, an intervention program to manage the bed bugs was implemented (199). While bed bug control was successful, there was no change in the incidence of childhood HBV rates, suggesting that bed bugs were not the major route of childhood HBV transmission.
In summary, the potential of HBV transmission via bed bugs is probably minimal. Perhaps, the risk of infection was always more perceived rather than real, since despite a considerable amount of research, there is no direct evidence to suggest that individuals have ever become infected with HBV through contact with bed bugs.
As for HBV, it was postulated that bed bugs may be involved in HIV transmission. It was observed that high rates of HIV infection occurred in children in parts of Africa where bed bugs were prevalent (190), and other explanations for the high rates had yet to be understood. Initial tests examining viral survival in bed bugs demonstrated that HIV could persist for up to 4 h in C. lectularius (161, 190). Attempts to transmit the virus via interrupted feeding did not occur, and it was concluded that HIV transmission was unlikely to happen in the normal human environment. A similar conclusion was found in a later study, whereby while HIV could be detected in bed bugs up to 8 days after oral exposure, HIV could not be detected in the feces, and no virus replication was found (315).
Within the insect order Hemiptera, to which bed bugs belong, the triatomine bugs from the family Reduviidae are known to transmit Trypanosoma cruzi, the etiological agent of Chagas' disease (169). The developmental cycle of this protozoan is relatively simple and occurs only within the gut of the insect. Transmission to humans results through contact with infected feces. In regions of South America where Chagas' disease is endemic, both bed bugs and triatomine bugs occur in the domestic environment. Thus, in light of the coexistence and relatedness of the bugs and the simple parasite developmental pathway, a number of field and laboratory investigations on the relationship between T. cruzi and bed bugs have been undertaken. Research up until the early 1960s was reviewed by Burton (55), and indications were that both C. lectularius and C. hemipterus were capable of acquiring and maintaining the parasite, and infectious stages could be transmitted in the feces. Since the review by Burton, several related articles have been published. An examination of beds in a region of Venezuela where Chagas' disease is endemic collected 138 C. hemipterus bed bugs, none of which had T. cruzi detected (the test methodology was not stated) (293). Those authors concluded that C. hemipterus would have a minor role, if any, in the transmission of T. cruzi in the domestic environment. In Argentina, C. lectularius bed bugs fed on wild-infected rodents were capable of transmitting T. cruzi and at an efficiency equivalent to that of triatomine bugs (159, 160). In those studies, T. cruzi was found to persist for more than 320 days in the bed bugs, and the complete developmental stages in the gut were observed via microscopy. Similar findings were recorded in another study for in another study C. lectularius infected with T. cruzi; there was complete parasite development within the gut, including the growth of the metacyclic infective stages, which were subsequently successfully transmitted to mice (69). Solid epidemiological or other evidence linking bed bugs with T. cruzi transmission within the domestic environment is currently lacking (127). However, it may be exceedingly difficult to differentiate the relative contribution to T. cruzi transmission in localities where both bed bugs and triatomine bugs coexist.
The current bed bug pandemic has again put bed bugs in the spotlight in terms of the potential to transmit human pathogens. A recent review of bed bugs and infectious diseases was published in 2011 by Delaunay and colleagues (82), who described some 45 pathogens as being potentially transmissible by bed bugs. Those authors also reviewed the vectorial potential of these pathogens, and thus, this information is largely not repeated herein.
Beyond HBV and T. cruzi, as described above, Delaunay and colleagues also reviewed the literature in relation to the possible transmission of Coxiella burnetii (the agent of Q fever) and fungi. For Q fever, data are very limited, with just one study suggesting that bed bugs may be capable of transmitting C. burnetii. Clearly, this information needs validation by other researchers, especially as C. burnetii is so readily transmitted by aerosols and other means (169). The fungi (and bacteria) detected on C. lectularius were all common environmental contaminants (251, 252), and there is no real suggestion that bed bugs may be transmitting these infections to humans. In fact, the risk may be to the female insect. Bed bugs undergo a complex mating behavior known as traumatic insemination, whereby the male's reproductive organ is modified to pierce the cuticle of the female abdomen to transfer sperm, thereby potentially introducing microbes (251).
One of the genera of bacteria listed by Delauny and colleagues, Wolbachia, includes symbiotic intracellular parasites of insects that are transmitted vertically. They are not passed by bed bugs through blood feeding and do not infect humans. The majority of bed bugs are naturally infected with Wolbachia as well as other endosymbionts (68, 154, 265). Considerable research has recently focused on various Wolbachia species, notably those that infect the dengue virus mosquito vector, Aedes aegypti (322). Infection in the mosquito can lead to a shortened life span or incompetence, ensuring that dengue virus is unable to complete development, and mass releases and the establishment of Wolbachia-infected mosquitoes into local populations may lead to a reduction in the incidence of human dengue virus infection. Releasing bed bugs into premises would not be popularly received, and thus, a similar approach could not be undertaken. In contrast to mosquitoes, studies have shown that the removal of Wolbachia has a negative impact on bed bugs; exposure to elevated temperatures kills the endosymbionts, leading to reduced fecundity (68). Whether such information could be practically employed to control infestations of bed bugs is yet to be ascertained.
Regarding other viruses, a reovirus from the ventriculus within the gut of the common bed bug, C. lectularius, was identified by electron microscopy (109). The origins of the bed bugs tested showing the presence of the virus were not stated in that study; the virus may have been acquired in a previous blood meal or could be an invertebrate virus. No further work on this virus has subsequently been reported. One group of researchers speculated that a virus may be present in the saliva of C. lectularius (110). Those researchers allowed bed bugs that had been gamma irradiated to repeatedly feed on rabbits, which induced the formation of skin papillomas. Those authors speculated that a virus was being transmitted, which was the cause of the clinical reaction in the rabbits. To date, this proposed virus has not been identified, nor have the results of the experiments been confirmed by others.
A recent letter to the editor attracted considerable media interest, as bed bugs were implicated as possible vectors of methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus faecium (VRE) (188). In that study, a sample of only five bed bugs was collected in Vancouver from a room infested with bed bugs (it was not stated if the residents had MRSA or VRE colonization or infections) and was tested for both bacterial strains. MRSA was isolated from three bed bugs (the species was not stated; it is possible that they could have been bat bugs), and VRE was isolated from two. Those authors surmised that as bed bugs feed and break the skin surface, there is a risk that such bacteria could be introduced. They concluded that this could be especially problematic in low-income housing, where hygiene standards are often lower and the levels of MRSA tend to be higher.
Perhaps, such findings should come as no surprise, considering the rates of antibiotic-resistant bacteria in the general community. In the United States, one study estimated that 1.5% of the population (or 4.1 million people) have MRSA nasal colonization (135). In an investigation of inpatients admitted to the hospital at a tertiary care center in Texas, 10.8% were found to be MRSA-positive nasal carriers (231). In Europe, it was estimated that 150,000 patients acquire MRSA infections annually (174). One study found that MRSA could readily survive for up to 8 weeks on a variety of fomites, indicating that many objects could serve as potential bacterial sources (83). MRSA is a very common organism, and the risk of potential exposure to the general community is high.
It was stated in the above-described letter that S. aureushas been reported to colonize the salivary glands of bedbugs for as long as 15 days (188), and those authors quoted a paper from the mid-1930s to strengthen their argument of the possible bed bug transmission of MRSA. To be exact, the original paper actually stated that, staphylococci were quite frequently discovered in smears of the salivary glands and of the contents of the intestine (112). Histological examination using specific markers to identify Staphylococcus within salivary cells was not undertaken (nor, presumably, were such techniques then available), and so the possibility of an environmental contamination of the smears cannot be discounted. There was no attempt to dissect out the salivary glands in the Vancouver study, but rather, whole-bug homogenates were tested, and so the presence of the bacteria externally on the bed bugs cannot be excluded. In light of modern knowledge on pathogen development in vectors, it would seem unlikely that Staphylococcus would progress to the salivary glands through the various inherent dissemination barriers within the insect (Staphylococcus bacteria are not known to undergo biological transmission in any vector). Thus, the discovery of a fairly ubiquitous bacterial strain on an urban pest should come as no real surprise. Again, as per most of the other pathogens mentioned above, a link between MRSA/VRE transmission and bed bugs is arguably possible but probably tenuous.
As inferred as described above, pathogens can be passed by arthropod vectors via either mechanical or biological transmission. In mechanical transmission, there is no development of the pathogen within the arthropod, whereas with the biological form, the pathogen matures and undergoes some amplification (295). Mechanically transmitted pathogens may be acquired during feeding and remain on the mouthparts to be passed onto another host in subsequent feeds or may be shed in the feces. It would appear that mechanical transmission is less efficient, principally because the pathogen must remain stable through a variety of environments. As there is no pathogen development, there may be little vector specificity (295).
In contrast, with biological transmission, a pathogen has to overcome certain dissemination barriers in order to undergo development within a vector; it has to be able to recognize each barrier, circumvent the barrier in order to pass through (i.e., have the right key for the right door), and then make it to the appropriate organ for replication. As a result, there tends to be high vector specificity with biological transmission. For example, for an arthropod-borne virus (arbovirus) to be transmitted through a bite, after the initial blood meal, the virus has to penetrate the midgut, escape into the hemocele (the arthropod's blood), infect the salivary gland, replicate, and then finally pass into the saliva during subsequent feeds (295). Arboviruses have evolved specific envelope proteins which recognize and overcome these barriers that otherwise limit the potential biological transmission of a pathogen.
Some pathogens undergo a simpler form of biological transmission. Trypanosomes develop in the gut of the insect and are passed in the feces. Similarly, the agent of murine typhus (Rickettsia typhi) also develops in the midgut and is shed in the feces (169). Even with this basic form of biological transmission, there are still barriers to infection that have to be overcome for the arthropod to be a competent pathogen vector.
Beyond these barriers, the environments within a warm-blooded host and that within an arthropod are extremely different. Human blood has a stable temperature and pH, whereas an arthropod's temperature is ostensibly the same as the ambient temperature. Any ingested pathogen has to be able to survive the different pHs of the bug's gut. Also, the pattern of blood cell digestion within hematophagous arthropods puts constraints on the ability of a vector to transmit a pathogen (304). Thus, vector-borne organisms have evolved to cope with these environmental changes.
As indicated above, there is no solid evidence yet to suggest that either C. lectularius or C. hemipterus is a competent vector of any pathogen. However, this is not the case for other members of the family Cimicidae. Swallow bugs (Oeciacus vicarious Horvath) are known to biologically transmit the arboviruses Fort Morgan virus (263), Buggy Creek virus (52), and Stone Lake virus (50) to swallow birds (Petrochelidon spp.). There is evidence to suggest that the arbovirus Kaeng Khoi virus can be transmitted to bats by the bat bugs Stricticimex parvus Ueshima and Cimex insuetus Ueshima (320). As other Cimicidae are capable of transmitting pathogens, then why not bed bugs?
The dissemination barriers and environmental differences, as discussed above, mean that many pathogens are simply unable to survive within the arthropod or to be transmitted. Recently, it was discovered that components of C. lectularius saliva include lysozyme and other peptides that are presumed to have antimicrobial activities (116). This may further reduce the ability of bed bugs to act as a vector. However, beyond the intrinsic factors within the vector, there are also various extrinsic variables that influence the possibility of an arthropod being able to transmit infectious agents of disease. Some of these variables may help to explain why bed bugs do not seem to be involved in pathogen transmission. Extrinsic factors include environmental factors that influence vector feeding behavior, host preferences by the vector, and the availability of appropriate vertebrate hosts. For the pathogen cycle to be completed, the vertebrate host must be able to become infected with the pathogen and then maintain it within the blood at a sufficient level and duration to infect other vectors (82, 295). If there are insufficient numbers of vertebrate hosts or insufficient numbers of immunologically nave individuals within the population, then pathogen transmission may not occur.
It is only in the relatively recent period of human history that individuals (and populations) have become highly mobile, largely through developments in transportation. Prior to the 1900s, most bed bug infestations would have been supported largely by a limited number of individuals, such as a single family group within a home. Many vector-borne pathogens involve a native vertebrate that acts as either a reservoir, an amplification host, or both. The lack of alternative vertebrate hosts and minimal host numbers may mean that it is difficult to sustain any vector-borne disease. While this is just speculation, perhaps computer modeling may give some credence to this hypothesis. In contrast, swallow and bat bugs would have the opportunity to feed on multiple individuals, and thus, there is a greater likelihood that a pathogen could be maintained within a population.
In reviewing the potential of bed bugs to transmit human disease agents, Goddard came to the conclusion, Even though bed bugs have been found naturally infected with many disease agents, they have never been proved to transmit even 1 (124, 125). It was correctly pointed out that the lack of evidence is not equivalent to the assumptions that bed bugs do not transmit disease (108). Of course, it is impossible to prove a negative, and, as such, this comment arguably has little scientific merit. Various authors suggested that further research is required to identify new pathogens and to examine the role of bed bugs in the transmission of infectious agents (82). Given that there is no evidence as yet that bed bugs have definitively transmitted any pathogen, what, then, is the risk?
Very few authors have attempted to quantify the overall number of infestations within a nation or the number of bed bugs within a single infestation, yet such information has direct relevance for the analysis of the risk of bed bugs potentially spreading infectious agents. From a survey of Australian professional pest managers in 2006, it was concluded that the overall number of bed bug infestations across the nation between the years 2000 and 2006 was conservatively estimated to be 100,000, with the year 2000 being around the time when the resurgence began to be evident (104). As the survey indicated that numbers of bed bug infestations were the highest in the year of the survey, presumably, by 2011, this number would have easily doubled (i.e., 200,000). In an apartment complex in Indianapolis, IN, the average numbers of bed bugs per infestation in two treatment groups were 103 and 507, while the median counts were 73.5 and 77 (309). As that study was undertaken in low-income housing, it could be argued that such numbers are higher than those at other sites. However, the cryptic nature of bed bugs means that it would not be possible to identify every individual, especially the juvenile stages, and the estimated numbers do not seem excessive in our experience.
Combining the estimated number of infestations in Australia in 2011 (200,000) with the lowest infestation count of 73.5 would give a total of 14.7 million individual bed bugs involved in the resurgence in Australia since the year 2000. If these figures are extrapolated to the United States, based on the United States having a human population of 300 million (about 15 times that of Australia, with around 20 million [318, 319]), a figure of 220.5 million bed bugs is obtained for the number of bed bugs involved in the resurgence in the United States since 2000. Of course, these figures are a very rough estimate, but they do provide an indication of the magnitude of the numbers of bed bugs since the resurgence began, and the overall worldwide figure obviously would be expected to be much higher still. It is not possible to prove that bed bugs cannot transmit any infectious agent; however, with over 200 million bed bugs biting (and biting multiple times), and without any evidence of any disease resulting, the indications are that the risk of contracting an infectious disease through the bite of a bed bug is almost nonexistent.
Arthropods that live in close association with humans produce a variety of allergens that can induce reactions and act as triggers for asthmatic attacks. Common domestic pests, including cockroaches (298), carpet beetles (155), and various acarines (notably the house dust mite [264]), have all been implicated in asthma, although exposure to any arthropod allergen could potentially lead to hypersensitivity (248). As bed bugs live in and around sleeping areas, the level of contact with the insects is high, and similar allergic and respiratory reactions have been recorded around the world (2, 157, 277, 312, 313). The control of bed bugs led to a subsequent reduction in the number of asthma attacks for an individual patient (277). Pest managers who undertake regular bed management have a risk of occupational exposure to bed bug allergens, with the potential development of hypersensitivity. This may be exacerbated by certain control activities, such as vacuuming, that could increase the amount of airborne allergens. The use of personal protective equipment (e.g., face masks) and vacuums with HEPA filters would reduce this risk.
In comparison to other hematophagous arthropods, bed bugs take a large blood meal, up to 13.9 mg (or 13.2 ml, with blood having a specific gravity of 1.0506 at 37C [294]), with an average of 7.81 mg (7.4 ml) for an adult female (297). As a consequence, when large numbers of bed bugs are present, anemia may occur. Excessive biting by bed bugs was implicated as the cause of iron deficiency in infants and children in Hyderabad, India (305), while severe anemia was reported in a 60-year-old patient, again with bed bugs being implicated as the cause (247). Robert Usinger, the author of the seminal work Monograph of Cimicidae, reported on his own declining hemoglobin levels as a result of maintaining a bed bug colony on himself (297). His hemoglobin levels declined from 14.5 g/10 ml of blood to 11.5 g over 5 years of feeding bed bugs and remained below normal levels despite supplementary iron intake. His hemoglobin levels rose to 13.2 g after several months following ceasing the feeding of the bugs.
It has been stated that bed bugs can produce an ill-defined syndrome that involves nervous disorders in sensitive people, and may contribute to the ill health of both children and adults (270). The original report was not cited, and thus, the etiology of the condition is uncertain. Despite this, the condition is often quoted.
Since the start of the bed bug resurgence, a number of indirect health impacts have become apparent. With the difficulty in controlling modern strains of bed bugs resistant to both pyrethroids and carbamates, people are undertaking extreme and desperate measures to control infestations, thereby putting their own and others' health at risk. For example, the use of rubbing alcohol to control bed bugs led to severe burns in one individual (120), and pest managers employing propane gas heaters have set homes and apartments on fire (20, 146), with one incident resulting in damages of Can$4.5 million (146). Fire fighters in New York have even found several incidences of people using highly volatile and inflammable liquids, such as gasoline, to control bed bugs (132).
The overuse and misuse of insecticides for bed bug control are becoming more common. Historically, extremely hazardous chemicals were used, including arsenic and mercury compounds, which were used as contact sprays, and hydrogen cyanide, which was employed as a fumigant, and human death did result (240). Products that currently are registered as safe for household use have much lower levels of mammalian toxicity; however, use not in accordance with label directions can pose a threat to health. Insecticide overuse is symptomatic of the high degree of resistance of bed bugs to most of the currently available insecticidal products. Some pest managers are now using illegal pesticides not registered for use against bed bugs (12), some of which are known to adversely affect the cognitive development of children (47), while a widely used but largely ineffectual pyrethroid (permethrin) can be highly toxic to cats (33). In mid-2011, a series of unexplained deaths in Chiang Mai, Thailand, were suggested to be the result of the overapplication of chorpyrifos (an organophosphate insecticide) to control bed bugs (21, 22, 59); however, the link has yet to be conclusively established. A CDC publication, which examined reports of acute illnesses associated with insecticide application against bed bugs from seven states between 2003 and 2010, identified 111 patients with adverse reactions and 1 fatality and a growing incidence over the period investigated (65). However, only 16% of these cases were categorized as being definitely or probably related to insecticide exposure (66), and the one fatality was a patient who had several predisposing serious medical conditions. Most of the adverse reactions were associated with pyrethroid or pyrethrin use (65).
Even in routine bed bug control, multiple applications of insecticides are usually required, which may expose the public to a greater risk of adverse reactions. There have been attempts in the United States to reregister compounds such as propoxur, which has a higher risk of toxicity to humans than currently available products. As yet, the U.S. Environmental Protection Agency (EPA), the government authority responsible for insecticide registration, has refused the registration application (41), and interestingly, insecticide resistance to this compound was recently reported for both the common and tropical bed bug species in Thailand (284). It is important that the hazard of a product relates to both its inherent toxicity as well as the risk of exposure (121). Perhaps, the targeted use of an effective product, albeit with a higher level of mammalian toxicity, may pose less of a risk than a less toxic product applied in much larger doses and on multiple occasions. This needs to be considered by insecticide registration authorities. Home-brew cocktails of various chemicals are now appearing on the Internet to control bed bugs (24), and the safety (and effectiveness) of such products is unknown. With the fears of insecticide misuse, the U.S. EPA and CDC released a joint statement in 2010 warning against the inappropriate application of products (64). Despite this warning, most respondents (93%) to a recent survey had little anxiety about insecticide applications to control bed bugs (246). It seems that the concern for most people is the eradication of the insect rather than the processes of achieving it.
Bed bugs have come to pose a threat to human health through other means. One of the busiest fire stations in Salt Lake City, UT, had to be temporarily closed for treatment as a result of staff being bitten by bed bugs (8). A shelter for the homeless in Franklin County, OH, had to close for 4 weeks due to bed bugs (205), forcing residents onto the street.
Bed bugs are even coming to threaten the provision of health services. For example, in Aurora, CO, a woman was refused medical treatment because her home was infested by bed bugs (23). The facility rejected the patient for fears that she may introduce bed bugs into the treatment rooms. On the basis of one patient thinking that she saw a single bed bug, a New York medical facility shut down an entire treatment floor (113). This response was somewhat premature, as none were found. In Kerry, Ireland, bed bugs led to a partial closure of a hospital for 2 weeks (253). In Australia, a whole wing of an adolescent ward of a major Sydney hospital in 2008 had to close down due to a severe bed bug infestation, with some 18 rooms being affected (104). In parts of the United States, the presence of even one bed bug in an intensive care unit will result in the unit being taken out of service for pest treatments (179). Bed bug infestations in hospitals are now becoming common (14), such that procedural guidelines to reduce the risk of bed bugs (13) and management protocols (152) are being developed. It is now clear that bed bugs are impinging upon human health in multiple ways as the insect is increasingly becoming a societal pest.
There are numerous reports of bed bugs impacting the mental health of individuals; however, these are largely anecdotal. Mental health impacts that are reported may include fatigue, distress, shame, anxiety, social isolation and stigma (235), exasperation, and irritation (18). A survey of 474 individuals with confirmed bed bug infestations in the United States during 2009 found that 22% of the respondents reported emotional stress, 20% stated that they had anxiety, and 14% had stress (241). In mid-May 2011, a presentation at the annual meeting of the American Psychiatric Association indicated that the mental health impacts of bed bugs can be far reaching (61), including a wide variety of affective, anxiety, and psychotic spectrum illnesses causing significant impairment, including suicidality and psychiatric hospitalization. Patients with previous mental issues can be further destabilized, while new patients can develop psychoses (61). Clearly, the mental trauma surrounding this pest is very real and cannot be ignored.
There is a social stigma associated with bed bugs, particularly as older articles published before the current resurgence painted a gloomy picture of the insect, typically associating it with poor housekeeping and hygiene (290). This public perception continues (61, 221, 239), and papers published even today often erroneously continue to associate poor hygiene with bed bugs (179). As a result, when people learn that there is an insect in their bed which is biting them at night, they are horrified and disgusted. Some people state that they feel dirty and unclean (92). For most, the bedroom is an inner sanctum for people to rest and unwind from the daily stresses of life, and to feel insecure in this highly intimate area of the home is understandably detestable. It is thus not surprising that in a recent survey, most people (99%) who had experienced bed bugs reported being upset and concerned (241). One pest manager who had to pacify many traumatized clients even quipped, rats, even V.D., is [sic] more socially acceptable than bedbugs (156). The psychological impacts of an infestation within the home has been investigated for other vermin and include depression, phobic anxiety, somatization [the conversion of anxiety into physical symptoms], hostility, and anomia [the inability to name objects] (324). There is no reason to suggest that bed bugs would not produce a similar spectrum of psychological responses.
Bed bugs can produce bite marks that can be very obvious and disfiguring if on the face and neck. This can interfere with peoples' employment and self-esteem. For example, in relation to impacting one's career, a nurse who was badly bitten in the staff accommodation block of a major Sydney teaching hospital was unable to attend patients, as it was feared that she had an infectious disease (92). An international athlete was sent home, as it was incorrectly assumed that she had chicken pox and could be infectious to other players (92). An actress was not given a movie role that required large parts of the body to be exposed, as she was heavily scarred from bed bug bites (92). A former guest of the Waldorf Astoria hotel in New York is seeking $10 million in compensation, claiming that plastic surgery is required to treat permanent scarring on the face after being heavily bitten by bed bugs (25).
This is an insect that is changing human behaviors; there is a report of people not using gym lockers in case they take bed bugs home (26). Charity workers are being prevented from their social efforts; volunteers who make quilts for veterans in Minneapolis are no longer having their donations accepted, again due to fears of bed bug transmission (53). A survey in early 2011 by the National Pest Management Association (NPMA), the peak industry body for pest managers in the United States, found that many Americans have modified their behavior due to the bed bug resurgence (220). Around one-quarter of respondents inspected or laundered their clothing after returning from travel, and a similar percentage inspected the hotel room. Some 17% examined their luggage upon return, while 12% cancelled or altered their travel plans. Of those who knew someone who had an infestation, 40% stated that they avoided entering the infested premise, and 33% discouraged those infested from entering their own homes.
People infested with bed bugs may become socially isolated. In Denver, CO, a patron of a local library was banned after bringing bed bugs into the building (10). The library even felt compelled to add further shame to the individual by publicly naming him. In a Facebook survey, 56% of people would abandon their date if bed bug bites were noticed on the skin, while 47% said that they would ask if their date had bed bugs before going back to their home (210). There are even instances where people have abandoned their dwelling to live in cars or tents to avoid nuisance bites (148). People with bed bugs often undertake fewer social interactions by not having friends and family to their home while the infestation is present (R. Cooper and S. L. Doggett, unpublished data). In the United Kingdom, one man lost his job as a result of sleeping at work, as he was unable to do so in his infested home, and his ex-wife refused to allow access to the children in case they acquired bed bugs (O. Madge, unpublished data).
Bed bugs are coming to disrupt everyday life, with all the associated inherent social and economic consequences. While they tend to be most often associated with homes and hospitality groups, bed bugs are turning up almost everywhere. Hospitals have been affected, resulting in ward closures and untreated patients; fire stations have closed; and the homeless have been forced back onto the street. Shopping stores have had to shut their doors (16, 180, 271), bugs have invaded office buildings (269), and iconic landmarks such as the Empire State building (268) and cinemas (104) are not exempt. Students' educations have been impacted: preschools have closed (15), and college dormitories have been evacuated for treatment (17). Aircraft have had to be grounded due to seats being infested (28). Bed bugs can be found virtually anywhere where people gather, from churches to brothels (104, 246). The widespread nature of infestations must be adding to community paranoia.
See the rest here:
Bed Bugs: Clinical Relevance and Control Options
- Bed Bugs! Yuck, Vancouver watch out! [Last Updated On: April 12th, 2010] [Originally Added On: April 12th, 2010]
- A Growing Problem in BC [Last Updated On: April 13th, 2010] [Originally Added On: April 13th, 2010]
- Shelters that house 600 scheduled to close next week – Vancouver Sun [Last Updated On: April 13th, 2010] [Originally Added On: April 13th, 2010]
- Blog: Bed Bugs in Downtown Vancouver Condos [Last Updated On: April 14th, 2010] [Originally Added On: April 14th, 2010]
- Bed Bugs in Downtown Vancouver Condos [Last Updated On: April 14th, 2010] [Originally Added On: April 14th, 2010]
- Viddler.com – Bed Bugs in Downtown Vancouver Condos – Uploaded by … [Last Updated On: April 15th, 2010] [Originally Added On: April 15th, 2010]
- Bed bugs in Regina; cost of thermal treatments coming down — Got ... [Last Updated On: April 19th, 2010] [Originally Added On: April 19th, 2010]
- Vancouver Island Getaway: Tofino & Victoria | Canada Forum ... [Last Updated On: May 16th, 2010] [Originally Added On: May 16th, 2010]
- Centre reopens after bedbug blitz – Vancouver Sun [Last Updated On: May 22nd, 2010] [Originally Added On: May 22nd, 2010]
- inFLIGHTout - San Francisco Bay Area: The Safety and Cleanliness ... [Last Updated On: May 31st, 2010] [Originally Added On: May 31st, 2010]
- Roy speaks about horrible living conditions in Vancouver Downtown ... [Last Updated On: June 6th, 2010] [Originally Added On: June 6th, 2010]
- Bed Bugs,Soon Coming to a Home Near you--or Perhaps Yours. [Last Updated On: June 11th, 2010] [Originally Added On: June 11th, 2010]
- How to avoid pests from home and yards? [Last Updated On: June 18th, 2010] [Originally Added On: June 18th, 2010]
- Rid of Bugs - Bed Bug Sniffing Dogs in the News – CBC Vancouver [Last Updated On: June 21st, 2010] [Originally Added On: June 21st, 2010]
- Winning Tactics to get rid of bed bugs [Last Updated On: June 21st, 2010] [Originally Added On: June 21st, 2010]
- Let your house be free from pests by various pest control mechanisms [Last Updated On: June 21st, 2010] [Originally Added On: June 21st, 2010]
- How To Fight Against Fleas In Your Home? [Last Updated On: June 21st, 2010] [Originally Added On: June 21st, 2010]
- Avoid troubles of frequent pests attack by using pest exterminator [Last Updated On: June 21st, 2010] [Originally Added On: June 21st, 2010]
- Troubles of repeated Termites invasion [Last Updated On: June 21st, 2010] [Originally Added On: June 21st, 2010]
- How to kill bed bugs | MNN - Mother Nature Network [Last Updated On: July 27th, 2010] [Originally Added On: July 27th, 2010]
- vancouver: Living With Bed Bugs [Last Updated On: August 7th, 2010] [Originally Added On: August 7th, 2010]
- Bed Bugs – everything you need to know article from USA Today ... [Last Updated On: August 20th, 2010] [Originally Added On: August 20th, 2010]
- How to Get Rid of Bed Bugs in Vancouver [Last Updated On: September 10th, 2010] [Originally Added On: September 10th, 2010]
- Does Bed Bug Resurgence Warrant Change in Tenant Screening? [Last Updated On: September 10th, 2010] [Originally Added On: September 10th, 2010]
- Beer, Bed Bugs and a Few First Impressions - Vancouver, Canada ... [Last Updated On: September 20th, 2010] [Originally Added On: September 20th, 2010]
- special education : [Last Updated On: September 28th, 2010] [Originally Added On: September 28th, 2010]
- Bed bugs continue infestation across North America - News1130 [Last Updated On: October 5th, 2010] [Originally Added On: October 5th, 2010]
- Bed bugs continue infestation across North America [Last Updated On: October 5th, 2010] [Originally Added On: October 5th, 2010]
- A New Tool To Gain the Upper Hand in Controlling Bed Bugs [Last Updated On: October 6th, 2010] [Originally Added On: October 6th, 2010]
- Bed Bugs in Vancouver | Vancouver Bed Bugs [Last Updated On: October 6th, 2010] [Originally Added On: October 6th, 2010]
- Parameters for picking up the right exterminator Vancouver [Last Updated On: October 6th, 2010] [Originally Added On: October 6th, 2010]
- What is bed bugs Vancouver and how to get rid of them? :ThaiBureau ... [Last Updated On: October 6th, 2010] [Originally Added On: October 6th, 2010]
- Gentrification in Vancouver BC [Last Updated On: October 8th, 2010] [Originally Added On: October 8th, 2010]
- Gentrification in Vancouver, Canada - Infoshop News [Last Updated On: October 8th, 2010] [Originally Added On: October 8th, 2010]
- How To Destroy Bed Bugs | Article Drop [Last Updated On: October 9th, 2010] [Originally Added On: October 9th, 2010]
- Learn exactly how to get rid of wasps [Last Updated On: October 9th, 2010] [Originally Added On: October 9th, 2010]
- Video: Bed bugs found at SFU | Metro Vancouver News Blog [Last Updated On: October 10th, 2010] [Originally Added On: October 10th, 2010]
- Video: Bed bugs found at SFU | Metro Vancouver News Blog « Bed ... [Last Updated On: October 10th, 2010] [Originally Added On: October 10th, 2010]
- Two dead in single car crash in southern B.C. | Metro Vancouver ... [Last Updated On: October 10th, 2010] [Originally Added On: October 10th, 2010]
- Simple Ways to Control Bed Bugs [Last Updated On: October 11th, 2010] [Originally Added On: October 11th, 2010]
- Dior Girl » News & Notes [Last Updated On: October 11th, 2010] [Originally Added On: October 11th, 2010]
- Blog Archive Company set to freeze out bed bugs – Coquitlam Now ... [Last Updated On: October 11th, 2010] [Originally Added On: October 11th, 2010]
- Blog Archive Bed bugs continue infestation across North America ... [Last Updated On: October 11th, 2010] [Originally Added On: October 11th, 2010]
- Blog Archive Bed bugs mean big business for Canadian distributor ... [Last Updated On: October 11th, 2010] [Originally Added On: October 11th, 2010]
- Ritzy Taste on a HoJo Budget « zona pellucida [Last Updated On: October 13th, 2010] [Originally Added On: October 13th, 2010]
- Bed Bugs in Vancouver – How to Prevent Them From Coming to You [Last Updated On: October 14th, 2010] [Originally Added On: October 14th, 2010]
- Bed bugs keep Calgary exterminators hopping [Last Updated On: October 18th, 2010] [Originally Added On: October 18th, 2010]
- Fruit Fly Larvae « Pest Control Company, Professional Exterminator … [Last Updated On: October 25th, 2010] [Originally Added On: October 25th, 2010]
- Winning Tactics to get rid of bed bugs | Getting Rid Of Bed Bugs [Last Updated On: October 25th, 2010] [Originally Added On: October 25th, 2010]
- Bedbug Infestation « Pest Control Company, Professional ... [Last Updated On: November 3rd, 2010] [Originally Added On: November 3rd, 2010]
- Bed Bugs in Downtown Vancouver Condos | Bed Bug Infestation [Last Updated On: November 3rd, 2010] [Originally Added On: November 3rd, 2010]
- Is It True That Bed Bug Infestations Are On The Rise? [Last Updated On: November 5th, 2010] [Originally Added On: November 5th, 2010]
- What Can You Do About Bed Bugs? [Last Updated On: November 5th, 2010] [Originally Added On: November 5th, 2010]
- Pest Control in Vancouver WA | Your Health Matters [Last Updated On: November 5th, 2010] [Originally Added On: November 5th, 2010]
- Pest Control in Vancouver WA « Get The Word Out [Last Updated On: November 5th, 2010] [Originally Added On: November 5th, 2010]
- Pest Control in Vancouver WA : CVN Money [Last Updated On: November 5th, 2010] [Originally Added On: November 5th, 2010]
- Pest Control in Vancouver WA « Linknet Video [Last Updated On: November 6th, 2010] [Originally Added On: November 6th, 2010]
- Alley Finds: Wood Side Table — Vancouver Is Awesome [Last Updated On: November 7th, 2010] [Originally Added On: November 7th, 2010]
- Hotels, landlords told bed bugs remain a threat [Last Updated On: November 8th, 2010] [Originally Added On: November 8th, 2010]
- Bed Bugs Creep Oe Out ! [Last Updated On: November 9th, 2010] [Originally Added On: November 9th, 2010]
- Good night, sleep tight: bed bugs have begun to bite in homes ... [Last Updated On: November 10th, 2010] [Originally Added On: November 10th, 2010]
- Bed Bug Registry | See videos, tweets and blogs on Bed Bug ... [Last Updated On: November 10th, 2010] [Originally Added On: November 10th, 2010]
- bed bug registry | Breaking News [Last Updated On: November 10th, 2010] [Originally Added On: November 10th, 2010]
- Bed Bugs in Downtown Vancouver Condos – 3237th Edition [Last Updated On: November 10th, 2010] [Originally Added On: November 10th, 2010]
- Bed Bugs are in Comforters « Pest Control Company, Professional ... [Last Updated On: November 11th, 2010] [Originally Added On: November 11th, 2010]
- Winning Tactics to get rid of bed bugs | Bed Bugs Signs [Last Updated On: November 14th, 2010] [Originally Added On: November 14th, 2010]
- Bed bugs are in Offices « Pest Control Company, Professional ... [Last Updated On: November 15th, 2010] [Originally Added On: November 15th, 2010]
- Steritech Launches SleepEasy™ Thermal Chamber to Quickly Kill Bed ... [Last Updated On: November 15th, 2010] [Originally Added On: November 15th, 2010]
- Steritech bed bugs - Beta Dao Blogs [Last Updated On: November 15th, 2010] [Originally Added On: November 15th, 2010]
- How to Avoid Costly Home Repairs - Walletpop Canada [Last Updated On: November 16th, 2010] [Originally Added On: November 16th, 2010]
- Pharisee church pastor calls bed bugs “God's wingless angels to ... [Last Updated On: November 20th, 2010] [Originally Added On: November 20th, 2010]
- Pharisee church pastor calls bed bugs “God's wingl - Blogspot [Last Updated On: November 20th, 2010] [Originally Added On: November 20th, 2010]
- Evolution of bed bugs [Last Updated On: November 20th, 2010] [Originally Added On: November 20th, 2010]
- Bed Bugs Vancouver [Last Updated On: November 23rd, 2010] [Originally Added On: November 23rd, 2010]
- Foam Mattresses Vancouver | Buy Mattresses Online | Huge Sale On ... [Last Updated On: November 26th, 2010] [Originally Added On: November 26th, 2010]
- Bed Bugs « Pest Control in Vancouver Wa – Peak Pest Management [Last Updated On: December 1st, 2010] [Originally Added On: December 1st, 2010]
- Welfare Wednesday – Vancouver, Canada - Eliminate Bed Bugs | Bed ... [Last Updated On: December 3rd, 2010] [Originally Added On: December 3rd, 2010]
- Pest control company help to exterminate carpenter ants [Last Updated On: December 6th, 2010] [Originally Added On: December 6th, 2010]
- Types of bedbugs and their control [Last Updated On: December 7th, 2010] [Originally Added On: December 7th, 2010]
- Types of bedbugs and their control « Door furniture, Brass door ... [Last Updated On: December 7th, 2010] [Originally Added On: December 7th, 2010]